The Vascular System as a Bioelectrical Interface: Palpitations, POTS, and Connective Tissue Divergence
Explore the vascular system as a bioelectric interface and potential health/clinical implications
CONNECTIVE TISSUEBIOLOGYSYSTEMS
Alexandra Chambers
6/17/202613 min read
Palpitations, tachycardia, dizziness, postural intolerance, internal tremor, venous pooling, heat sensitivity, faintness, and collapse-like symptoms are often interpreted through a narrow clinical framework. They may be described as anxiety, stress, deconditioning, hydration failure, benign palpitations, or unexplained autonomic symptoms. Although these categories may describe part of the downstream presentation, they do not fully account for the biological systems through which circulation, electrical signalling, vascular tone, salt-water balance, and sensory-autonomic regulation are maintained.
This article proposes that the vascular system should also be examined as an embodied connective-tissue and bioelectrical phenomenon. Before a palpitation is experienced as a cardiac event, the body has already engaged multiple systems: veins, arteries, electrolytes, blood volume, renal salt handling, autonomic signalling, immune mediators, mitochondrial energy, ion channels, and connective tissue architecture. The heart does not beat in isolation. It beats inside a vascular system whose mechanical and biochemical conditions determine how hard it must work to maintain circulation.
A connective tissue framework does not replace cardiology, neurology, or autonomic medicine, it situates them within a broader biological pathway. If the vascular system is structurally divergent, the heart may be required to compensate electrically. If blood volume is insufficient, salt and water are poorly retained, electrolytes are unstable, or the autonomic nervous system is triggered by illness, inflammation, heat, sensory load, or immune activation, the rhythm of the heart may become the visible output of a deeper regulatory burden.
Palpitations should therefore not be treated as meaningless simply because they are internally felt. Like pain, dizziness, nausea, or breathlessness, palpitations are experienced from within the body. The correct clinical question is what physiological event corresponds to that sensation. Without rhythm capture, electrolyte assessment, autonomic context, medication review, and attention to vascular mechanics, attributing palpitations to anxiety risks becoming interpretation rather than evidence.
This framing has particular relevance for divergent populations because dysautonomia, migraine, sensory sensitivity, fatigue, hypermobility, mast-cell reactivity, epilepsy, gastrointestinal dysmotility, medication sensitivity, and connective-tissue variation often overlap. These presentations are commonly divided between separate clinical specialisms. The nervous system is treated as neurological, the heart as cardiological, the vessels as circulatory, the skin and joints as connective tissue, and distress as psychological. Yet the body itself does not operate in separate departments; electrical stability is produced through the interaction of systems.
The Heart
The heart is an electrically excitable organ; every heartbeat depends on coordinated depolarisation and repolarisation of cardiac cells, driven by the movement of ions across cell membranes. The heart’s rhythm is therefore mechanical, electrical, ionic, metabolic, and autonomic. The electrocardiogram records electrical activity, and the timing of each beat depends on membrane voltage, sodium movement, calcium signalling, potassium repolarisation, magnesium regulation, pacemaker activity, conduction pathways, and autonomic input. The heart is a frequency-dependent organ whose rhythm is shaped by internal and external conditions.
Heart rate, heart-rate variability, conduction timing, respiratory sinus arrhythmia, autonomic oscillation, and repolarisation intervals all involve rhythmic repetition over time. Frequency means repetition per unit of time; sound, light, breath, movement, circadian rhythm, and neural firing all involve frequency. However, in excitable tissues such as the heart and brain, frequency is inseparable from electrical behaviour. Cardiac cells generate repeated electrical action potentials. Neurons fire in rhythmic patterns. Seizures represent dysregulated synchronised electrical activity in neural networks. Arrhythmias represent dysregulated electrical rhythm in cardiac tissue.
This is where the term electrical vulnerability becomes useful. Electrical vulnerability can be used as a systems-level descriptor for bodies whose excitable tissues operate closer to threshold because of inherited, acquired, metabolic, immune, structural, electrolyte, pharmacological, or environmental factors. In this framework, palpitations, POTS, migraine, epilepsy, sensory overload, internal tremor, and dysautonomia are not identical conditions, but they may share one principle: reduced tolerance across electrically active systems.
Electrolytes and the Mineral Language of Bioelectricity
The term electrolyte itself reveals the mechanism; electrolytes are electrically active ions in body fluids. They are not merely hydration salts or nutritional extras. They are part of the body’s electrical infrastructure. Sodium, potassium, calcium, magnesium, chloride, bicarbonate, and phosphate help maintain membrane voltage, nerve signalling, muscle contraction, vascular tone, fluid balance, and cardiac rhythm.
The heart depends on electrolytes because cardiac rhythm is produced through ion movement. Sodium contributes to rapid depolarisation, calcium links electrical signalling to contraction, and potassium is central to repolarisation and resting membrane potential. Magnesium modulates excitability and interacts with calcium and potassium physiology. Chloride and bicarbonate participate in acid-base and cellular electrical balance. If electrolyte balance is unstable, the electrical threshold of the heart may shift.
For the individual, this may present as palpitations, ectopic beats, tachycardia, weakness, tremor, dizziness, internal vibration, muscle twitching, migraine, seizure vulnerability, or rhythm irregularity. These symptoms may be interpreted as stress, anxiety, or panic. However, from a bioelectrical perspective, they may reflect altered conductivity within the body’s internal fluid system.
From a divergent genomics perspective, electrolyte instability should not be reduced to inadequate water intake. In some bodies, it may reflect altered sodium retention, potassium handling, aldosterone signalling, renal transport, vasopressin response, connective-tissue-mediated vascular pooling, mast-cell mediator effects, medication sensitivity, mitochondrial strain, gastrointestinal loss, or autonomic dysregulation. If the heart is an electrical organ, then electrolytes are part of the cardiac signalling system itself.
The Vascular System
Blood vessels are living connective-tissue structures. Veins and arteries contain extracellular matrix proteins, including collagen and elastin, alongside smooth muscle, endothelial cells, autonomic nerves, immune-responsive tissue, and pressure-sensitive signalling systems. These structures influence how vessels stretch, recoil, constrict, dilate, and tolerate pressure.
This is where connective-tissue divergence becomes mechanistically important. If collagen and extracellular matrix architecture vary, vascular mechanics may also vary. In some bodies, veins may be more compliant or more distensible: able to stretch, but less able to recoil and return blood efficiently. This means that veins may be mechanically over-compliant or poorly supported.
When upright, poorly supported veins may allow more blood to pool in the lower body. This reduces effective venous return to the heart. The heart can only pump out what returns to it. When less blood returns, the heart fills less between beats and pumps out less blood with each beat. This is called reduced stroke volume, and to preserve blood flow to the brain and body, the autonomic nervous system may drive the heart rate upward.
The mechanism can be summarised as follows:
connective tissue / collagen / extracellular matrix divergence
→ increased venous compliance or reduced vascular recoil
→ blood pooling and reduced venous return
→ reduced stroke volume
→ sympathetic compensation
→ tachycardia and palpitations.
This is one of the most important mechanisms in a divergent genomic model of POTS and palpitations. The heart is the organ forced to compensate for vascular-connective-tissue instability.
POTS as Electrical Compensation
Postural orthostatic tachycardia syndrome, or POTS, is usually defined clinically by a sustained rise in heart rate after standing, without the blood-pressure drop seen in classical orthostatic hypotension. Symptoms may include palpitations, dizziness, light-headedness, tremor, fatigue, brain fog, chest discomfort, weakness, nausea, heat intolerance, exercise intolerance, and collapse-like episodes.
However, this definition describes the visible output. It does not fully explain the underlying mechanism. POTS is better understood as the cardiovascular expression of upright regulation failure. When a person stands, gravity pulls blood downward into the legs and abdomen. The body must rapidly coordinate venous return, vascular constriction, heart rate, stroke volume, baroreflex signalling, autonomic tone, blood volume, electrolyte balance, and cerebral perfusion.
If that coordination fails, the heart may accelerate in an attempt to preserve blood flow to the brain. POTS can therefore be understood as a compensatory electrical response to mechanical, vascular, autonomic, immune, salt-water, electrolyte, or metabolic instability. The heart becomes louder because the body is struggling to maintain stable circulation under gravitational stress.
A fast heart rate is not automatically anxiety - tachycardia is a rate - arrhythmia is a rhythm disturbance. Palpitations are the lived experience of force, speed, fluttering, irregularity, skipping, pounding, or internal cardiac disturbance. Anxiety can influence heart rate and autonomic tone, but it should not be used as a shortcut explanation for palpitations. Without rhythm capture, anxiety is often an interpretation rather than evidence.
Salt, Water, and the Genomics of Blood Volume
The heart beats within a vascular system whose effectiveness depends not only on vessel structure, but on circulating volume. Blood volume is maintained through renal sodium handling, aldosterone signalling, vasopressin-mediated water retention, electrolyte balance, vascular tone, and autonomic feedback. If these systems are unstable, the heart may be forced to compensate electrically.
This is particularly relevant in POTS, where the visible feature is tachycardia but the underlying mechanism may include hypovolaemia: insufficient effective circulating volume. In typical physiology, reduced blood volume should activate the renin-angiotensin-aldosterone system, increasing sodium and water retention. However, some POTS research has described a renin-aldosterone paradox in which low blood volume is not matched by an appropriately compensatory aldosterone response. This suggests that blood-volume regulation, renal signalling, and sodium conservation may be central to the condition in at least a subset of patients.
Sodium and water balance are biologically regulated traits. Aldosterone signalling depends on mineralocorticoid receptor function and epithelial sodium channels. Renal salt transport depends on sodium, potassium, and chloride transporters. Water retention depends on vasopressin signalling and aquaporin channels. Significant disruption of these pathways produces recognised salt-wasting or water-wasting disorders, but mild variation may still influence physiological resilience.
Relevant genomic pathways include mineralocorticoid receptor signalling, epithelial sodium channels, renal salt transporters, vasopressin receptors, aquaporins, and renin-angiotensin-aldosterone regulation. Genes such as NR3C2, SCNN1A, SCNN1B, SCNN1G, SLC12A1, SLC12A3, KCNJ1, CLCNKB, AVPR2, AQP2, ACE, AGT, AGTR1, and CYP11B2 sit within or adjacent to these systems. The point is that salt and water retention are genetically regulated, and variation in these systems may contribute to vulnerability in subgroups.
This creates a two-part mechanism.
Connective-tissue divergence may alter the vascular container: veins may be more compliant, more distensible, or less able to recoil and return blood efficiently when upright.
Salt and water-handling divergence may alter the volume inside that container. A body with increased venous compliance and reduced effective circulating volume is placed in a chronic compensation state. The heart must beat faster to preserve cerebral perfusion.
The heart may be electrically unstable because the body is volumetrically unstable.
A Non-linear Vascular-Connective-Tissue Spectrum
Connective tissue should not be interpreted as a binary claim in which a person either has a diagnosable connective-tissue disorder or has no connective-tissue-mediated vascular vulnerability at all. It is better understood as a non-linear spectrum shaped by genetic variation, gene expression, epigenetic regulation, hormonal state, mechanical load, inflammation, nutrition, ageing, injury, and environmental exposure.
Clinically significant presentations exist, such as vascular Ehlers-Danlos syndrome (EDS), where pathogenic variants affecting type III collagen can produce arterial, organ, and tissue fragility. These conditions demonstrate, in the clearest possible way, that collagen biology is inseparable from vascular integrity. However, vascular EDS should not be treated as the only meaningful expression of connective-tissue vascular involvement. It is the extreme condition, not the whole map.
Across the wider spectrum, less formally recognised connective-tissue variation may still influence vascular mechanics. Some individuals may present primarily with joint hypermobility, skin features, easy bruising, sensory sensitivity, gastrointestinal dysmotility, migraine, dysautonomia, POTS, venous pooling, temperature intolerance, palpitations, or fatigue. Others may have only partial features, but this can be missed clinically and can still be impactful on health. This variability is not a contradiction of the model; it is what would be expected from non-linear genomic expression.
The absence of vascular EDS does not mean the absence of vascular connective-tissue involvement. Severe collagen disorders reveal the principle; milder divergent expression reveals the spectrum.
A person may not look hypermobile, may not identify as bendy, and may not show obvious external signs, while still carrying variation in collagen, extracellular matrix organisation, vascular compliance, fascia, epithelial barriers, or autonomic support structures. The absence of visible hypermobility does not exclude connective-tissue involvement; it only means connective tissue is not presenting through the most obvious external route.
The same broad connective-tissue logic that may affect the eyes, ears, fascia, skin, joints, gut, and sensory structures also likely affects the cardiovascular system. The difference is where, how strongly, and under what conditions it becomes clinically visible.
Venous Access and Blood Draw Difficulty
Difficulty with blood draws may provide a small but revealing example of vascular connective-tissue divergence. Veins are living connective-tissue structures, therefore collagen and extracellular-matrix variation may influence not only orthostatic circulation, but also practical venous access. In some individuals, veins may be more mobile, more collapsible, more fragile, more poorly supported by surrounding tissue, or more prone to bruising after puncture.
This would not apply universally, and it would not make every difficult blood draw a collagen issue. However, on a nonlinear spectrum of connective-tissue expression, it is biologically plausible that the same vascular mechanics involved in venous pooling, reduced recoil, and orthostatic intolerance could also make routine venepuncture more difficult.
If the veins behave differently when standing, it is not unreasonable to ask whether they may also behave differently when punctured.
Blood draw difficulty may also involve low circulating volume, dehydration tendency, autonomic vasoconstriction, sensory sensitivity, pain amplification, medical trauma, and vasovagal physiology. These mechanisms can converge in the same moment: a difficult vein, a stressed autonomic system, and an overwhelmed nervous system. The procedure is then misread as fear alone, when the underlying issue may be vascular, autonomic, sensory, and connective-tissue mediated.
Multiple Routes Into POTS-Like Physiology
Connective tissue is one prominent convergent pathway into POTS-like physiology. Some people may have a vascular-container problem, where compliant veins and altered extracellular matrix allow blood to pool when upright. Others may have a volume problem, where salt and water are not retained efficiently enough to maintain stable circulating volume. Some may have an autonomic signal problem, where the nerves controlling vascular constriction do not respond appropriately.
It can also be linked to a hyperadrenergic problem, where excessive sympathetic activation or impaired catecholamine clearance produces tachycardia, tremor, sweating, and internal agitation. Some cases may have an immune-triggered problem, where infection, inflammation, mast-cell activation, autoantibodies, or post-viral dysregulation destabilise the autonomic system. Others may have an energetic or electrical threshold problem, where mitochondrial strain, electrolyte instability, ion-channel variation, migraine vulnerability, seizure vulnerability, or medication sensitivity lowers the body’s capacity to maintain stable signalling.
These mechanisms can overlap and converge. One person may have mild connective-tissue divergence, low effective blood volume, electrolyte sensitivity, mast-cell activation, and autonomic instability at the same time. Another person may have no visible connective-tissue features at all, but develop POTS-like symptoms after infection because inflammation, fever, dehydration, immune activation, and sympathetic stress have disrupted autonomic regulation.
This fits the non-linear spectrum model. The same outward symptom - palpitations, tachycardia, dizziness, tremor, brain fog, heat intolerance, or collapse-like episodes - may arise through different biological routes.
POTS-like symptoms may therefore represent a final common pathway: different mechanisms converging on unstable upright circulation and compensatory cardiac acceleration.
Voltage-Gated Channels and Excitable-System Thresholds
Discussion of electrical vulnerability must include ion channels. The heart, brain, vascular smooth muscle, gut, skeletal muscle, endocrine tissues, and autonomic networks all depend on excitable membranes, ion gradients, and calcium signalling. Voltage-gated calcium channels are particularly important because they sit at the interface between membrane voltage and cellular behaviour. When the membrane depolarises, calcium enters the cell and can trigger neurotransmitter release, muscle contraction, vascular tone, hormone secretion, immune activation, gene expression, and mitochondrial response.
This makes calcium-channel biology a bridge between the nervous system, heart, vascular system, endocrine system, immune system, and metabolic function. In some neurodivergent subgroups, evidence implicating calcium-channel genes, glutamate-GABA balance, NMDA receptor function, magnesium gating, and ion-channel regulation suggests that excitable tissues may operate closer to threshold.
This means that some divergent bodies may carry altered regulation of excitable membranes. Their thresholds may therefore be altered. If calcium-channel regulation, glutamate signalling, GABAergic inhibition, magnesium gating, mitochondrial energy, or electrolyte balance is shifted, the body may become less able to stabilise signalling under stress.
Pharmacogenomically, this has major implications. Medication response cannot be interpreted only through diagnosis. Drugs that affect calcium-channel subunits, glutamate signalling, GABAergic tone, catecholamines, cardiac repolarisation, electrolytes, vascular tone, blood pressure, or drug metabolism may have disproportionate effects in people whose electrical regulation is already unstable. A medication may be standard on paper while becoming destabilising in a body with low blood volume, autonomic dysfunction, altered electrolyte handling, mitochondrial vulnerability, POTS, seizure history, mast-cell activation, or connective-tissue vascular involvement.
Clinical Reductionism and the Cost of Psychologising Symptoms
Triage is necessary; however, the problem is when triage becomes reductionism. If palpitations are not immediately dangerous, they may be treated as unimportant. If ECG findings are not captured during the episode, symptoms may be dismissed. If a person is young, marginalized, neurodivergent, hypermobile, chronically ill, traumatised, or visibly distressed, the likelihood of psychologization increases.
This produces an epistemic failure; the absence of immediate emergency findings is not the same as the absence of physiological dysfunction. Many forms of dysautonomia, POTS, mast-cell activation, intermittent arrhythmia, metabolic instability, medication sensitivity, salt-water dysregulation, and connective-tissue-mediated vascular dysfunction are episodic. They may not be visible during a brief appointment. A body can be unstable in real life while appearing unremarkable in a static clinical snapshot.
A progressive model would ask what happens to this person when upright, hot, unwell, fasting, menstruating, over-exerted, sensory-overloaded, medicated, dehydrated, sleep-deprived, electrically exposed, or immune-triggered. It would ask whether the heart is racing because the vascular system is failing to return blood, whether electrolytes are unstable, whether there is hypovolaemia, whether the person is hyperadrenergic, whether connective-tissue divergence is present, whether mast-cell symptoms coexist, whether there are seizure, migraine, or sensory-excitability patterns, and whether medication effects, thyroid function, iron status, blood count, electrolytes, and family history have been properly considered.
These questions avoid invalidation of the individual and their experience; they also assume competence, and arguably most importantly - they assume physiology.
Omission From Diagnostic Frameworks
The physiology described here is well-known and scattered across academic papers. Vascular involvement is recognised clinically in diagnosed connective-tissue disorders, and POTS is recognised as a disorder of orthostatic heart-rate regulation. Electrolytes are recognised as clinically relevant to cardiac rhythm. Salt and water regulation are recognised as renal and endocrine processes. Ion channels are recognised in arrhythmia, epilepsy, migraine, neurodevelopment, and pharmacological response. Mast-cell mediators, immune activation, and infection are recognised as capable of affecting vascular and autonomic function.
The problem is not the absence of biological knowledge, but the failure of integration. These mechanisms are not brought together within neurodivergence, sensory sensitivity, dysautonomia, chronic fatigue, migraine, hypermobility, mast-cell activation, medication sensitivity, or palpitations frameworks in a systematic way. Instead, symptoms are commonly divided into separate diagnostic compartments or interpreted through psychological categories when standard testing does not immediately reveal a severe cardiac abnormality.
Cross-disciplinary thinking between genomics, cardiology, vascular biology, autonomic medicine, nephrology, neurology, immunology, pharmacogenomics, connective-tissue medicine, mitochondrial biology, and environmental health is necessary. It would also require recognition that divergent physiology should not be reducible to subjective intolerance. The body maintaining circulation may be structurally, electrically, volumetrically, and immunologically different.
Conclusion
Vascular and electrical instability in divergent populations should not be understood as a purely cardiac problem, a purely psychological problem, or a purely neurological problem. The heart is a bioelectrical organ held within a vascular, connective-tissue, electrolyte, renal, immune, endocrine, autonomic, and metabolic network. If any part of that network becomes unstable, the heartbeat may become the signal through which the body reveals its burden.
POTS offers a clear example. Its recognisable sign is cardiac, but its mechanisms may include venous pooling, hypovolaemia, reduced vascular recoil, connective-tissue laxity, small-fibre neuropathy, hyperadrenergic signalling, mast-cell activation, salt-water dysregulation, immune triggers, electrolyte instability, mitochondrial strain, and altered ion-channel thresholds. The heart races not because the person is weak, dramatic, or emotionally excessive, but because the body is attempting to preserve perfusion under unstable conditions.
Palpitations are not always dangerous, but they are also not meaningless. They are signals from an electrically active body attempting to maintain coherence across multiple regulatory systems.
The vascular system is a connective-tissue and bioelectrical interface. Veins, blood volume, electrolytes, autonomic tone, immune signalling, and cardiac rhythm all participate in the same regulatory ecology. To understand palpitations and POTS-like symptoms in divergent bodies, medicine must move towards an integrated systems model of electrical vulnerability.
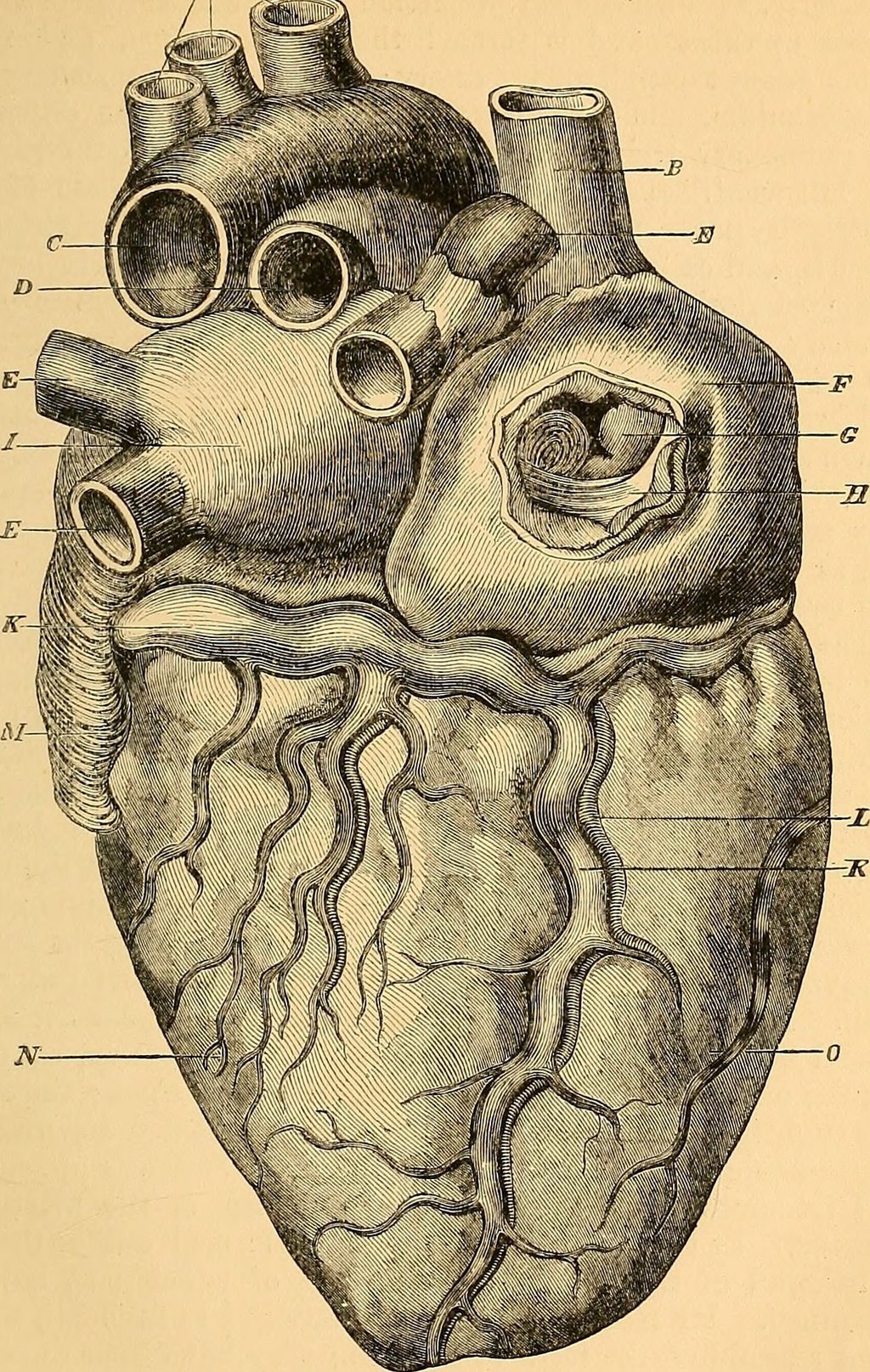
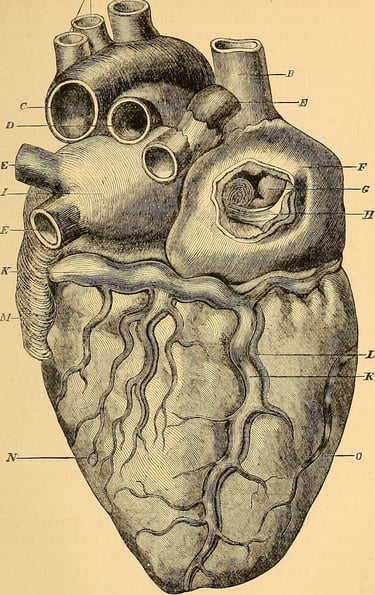
Artist: john Hatch Power, Anatomy of the arteries of the human body; descriptive and surgical, with the description of the heart (Dublin: Fannin; London; longmans, 1881).
Contact
Reach out with questions or collaboration ideas.
AChambers@divergentgenomics.org
© Alexandra Chambers 2026. All rights reserved.